Asthma is a common chronic respiratory condition that nurses frequently encounter in both outpatient and inpatient settings. Effective medication management is essential for controlling symptoms, preventing exacerbations, and improving long-term respiratory health. In this episode, we’ll review the major medication classes used to manage asthma and highlight key nursing considerations when caring for patients with this condition.
In this episode, we are going to review antiarrhythmic drugs that clinicians may encounter in practice: Digoxin, Propafenone, Dofetilide, and a few others. While these drugs are commonly used in the management of atrial fibrillation and other rhythm disturbances, they each come with important pharmacology and safety considerations that pharmacists and healthcare providers need to recognize.
Digoxin is a cardiac glycoside that increases contractility while also slowing AV node conduction through enhanced vagal tone, making it useful for rate control in atrial fibrillation, particularly in patients with heart failure. However, it has a narrow therapeutic index, and toxicity can occur if renal function declines or electrolyte abnormalities develop.
Propafenone is a Class IC sodium channel blocker used primarily for rhythm control in atrial fibrillation. A key clinical pearl with this medication is that it should generally be avoided in patients with structural heart disease due to the risk of proarrhythmia.
Dofetilide and sotalol are both Class III antiarrhythmics that work by blocking potassium channels and prolonging cardiac repolarization. Because of their ability to prolong the QT interval, both agents carry a risk of torsades de pointes and require careful monitoring. Dofetilide initiation typically requires hospitalization to monitor the QT interval and adjust dosing based on renal function. Sotalol also requires attention to renal function and ECG monitoring, and it has additional beta-blocking effects that can contribute to bradycardia and fatigue.
Throughout this episode, we will break down the mechanisms, common clinical uses, and key safety pearls for these medications to help you better understand how they fit into arrhythmia management.
Antiarrhythmic medications are some of the most complex and high-risk drugs pharmacists encounter in clinical practice. In this episode, we break down the most important concepts pharmacists need to understand about antiarrhythmics, including the major drug classes and the clinical situations where these medications are commonly used.
A major focus of the discussion is medication safety. Many antiarrhythmics carry risks such as QT prolongation, proarrhythmia, and significant drug–drug interactions. Pharmacists play a critical role in identifying these risks, monitoring electrolytes and ECG changes, and recognizing situations where therapy adjustments are necessary. We also highlight why certain medications require inpatient initiation and careful monitoring.
The episode also covers practical clinical pearls, including the unique toxicity profile and interaction potential of amiodarone, how to think about rate control versus rhythm control strategies in atrial fibrillation, and the most common medication-related problems pharmacists should watch for. Whether practicing in ambulatory care, hospital, or long-term care settings, understanding antiarrhythmics can help pharmacists prevent serious complications and improve patient outcomes.
P2Y12 inhibitors are a cornerstone of antiplatelet therapy in cardiovascular disease. These agents block the P2Y12 receptor on platelets, preventing ADP-mediated activation and reducing platelet aggregation. By inhibiting this amplification pathway, they help prevent arterial thrombosis in conditions such as acute coronary syndrome, percutaneous coronary intervention, stroke, and peripheral artery disease. The most commonly used oral agents include clopidogrel, prasugrel, and ticagrelor, each with important pharmacokinetic and clinical differences that influence agent selection.
From a pharmacist’s perspective, choosing the right P2Y12 inhibitor requires balancing ischemic benefit with bleeding risk. Clopidogrel requires CYP2C19 activation and is subject to drug interactions and genetic variability. Prasugrel provides more potent inhibition but carries a higher bleeding risk and is contraindicated in patients with prior stroke or TIA. Ticagrelor offers reversible inhibition but comes with unique considerations such as dyspnea and drug interactions via CYP3A4. Understanding these nuances allows pharmacists to optimize dual antiplatelet therapy and improve patient outcomes.
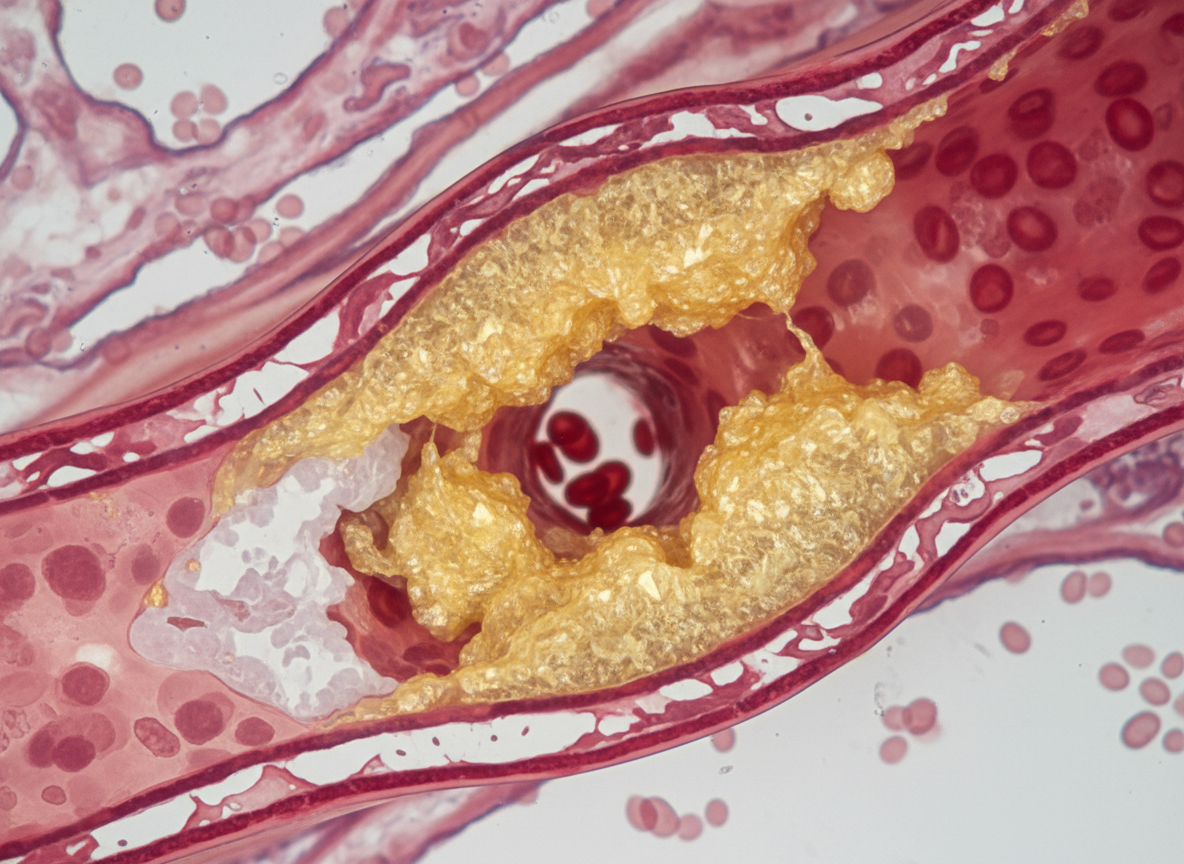
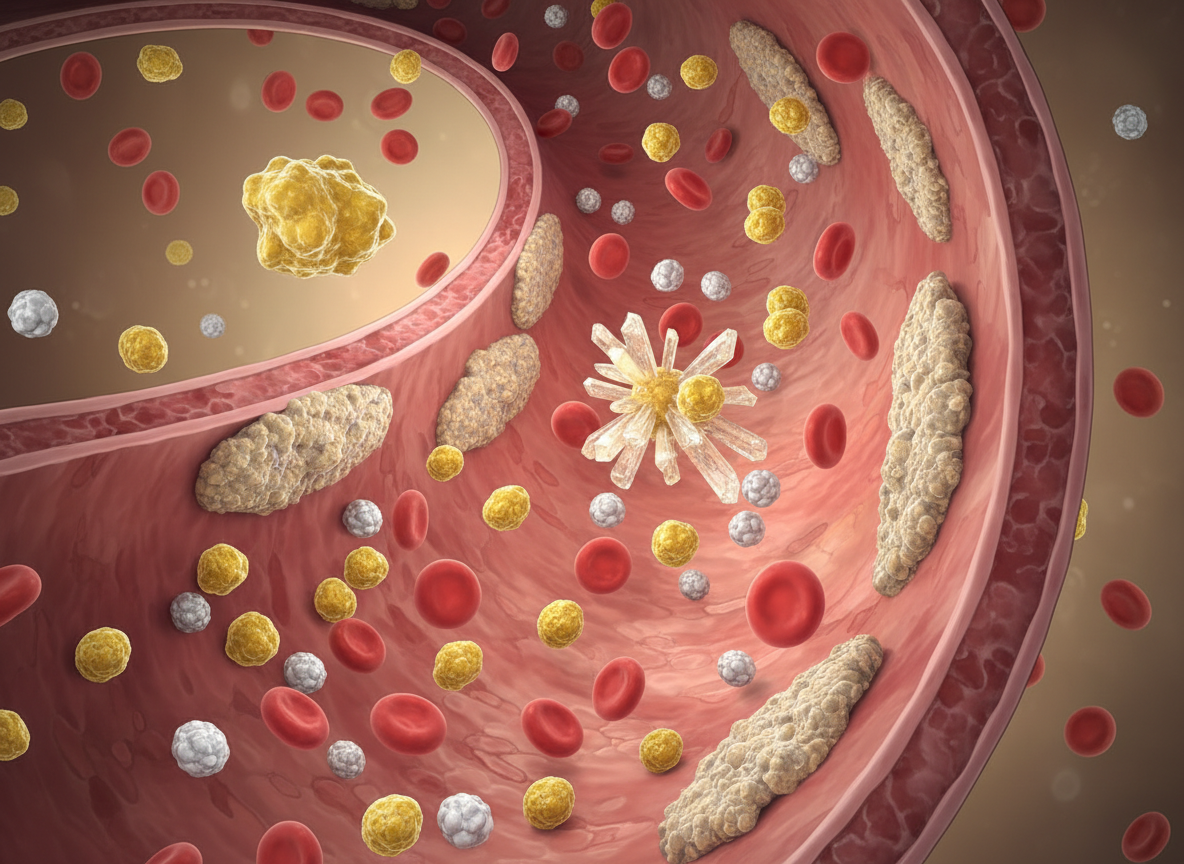
Managing cholesterol is a key part of preventing cardiovascular disease, and nurses are on the front lines of patient care. In this episode, we explore the main cholesterol-lowering medications, including statins, ezetimibe, PCSK9 inhibitors, fibrates, and more. You’ll learn how each medication works, important side effects, lab monitoring, and nursing considerations for safe administration. We’ll also cover strategies for educating patients and supporting long-term adherence. By the end of this episode, you’ll have practical tools to confidently recognize, monitor, and teach about cholesterol medications in everyday nursing practice.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse
Heart failure management has evolved dramatically, and nurses are central to optimizing outcomes and preventing hospital readmissions. In this episode, we break down the core medication classes used in heart failure, including ACE inhibitors, ARBs, beta blockers, mineralocorticoid receptor antagonists, diuretics, and newer agents like ARNIs and SGLT2 inhibitors. You’ll learn how these medications improve symptoms and survival, key monitoring parameters such as blood pressure, potassium, and renal function, and common adverse effects to watch for. We’ll also review practical bedside considerations and patient education pearls that improve adherence and safety.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse
Heparin medications are commonly used in hospitals, and nurses play a critical role in ensuring they’re given safely. In this episode, we break down unfractionated heparin and low molecular weight heparins in a practical, easy-to-understand way. We’ll also review dosing considerations, signs of bleeding, and the importance of recognizing heparin-induced thrombocytopenia early. Plus, we’ll cover reversal with protamine and essential patient safety tips. Whether you’re preparing for exams or managing anticoagulation at the bedside, this episode will help you confidently navigate heparin therapy in clinical practice.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse
Anticoagulation therapy can feel complex, but nurses play a vital role in keeping patients safe. In this episode, we break down the key differences between warfarin and direct oral anticoagulants (DOACs), including how they work, when they’re used, and what makes each unique. You’ll review important monitoring parameters like INR for warfarin, renal function considerations for DOACs, major drug and food interactions, and bleeding risk assessment. We’ll also cover reversal strategies and practical patient education pearls. Whether you’re preparing for exams or managing patients on anticoagulation, this episode will simplify the essentials and strengthen your confidence in safely caring for patients on warfarin and DOAC therapy.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse
Atrial fibrillation is one of the most common cardiac arrhythmias nurses encounter, and understanding its management is essential for safe patient care. In this episode, we break down what atrial fibrillation is, why it increases stroke risk, and how treatment strategies focus on rate control, rhythm control, and anticoagulation. We’ll review common medications, monitoring priorities, and key assessment findings you should never ignore.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse
Hypertension medications are a cornerstone of nursing practice, and understanding how they work can dramatically improve patient safety and outcomes. In this episode, we break down the major antihypertensive drug classes, including ACE inhibitors, ARBs, beta blockers, calcium channel blockers, and diuretics, in a practical and easy-to-understand way. You’ll learn how each class lowers blood pressure, key monitoring parameters, common side effects, and important nursing considerations. We’ll also cover when to hold medications, what lab values matter most, and how to educate patients to improve adherence.
Your support helps me provide more free resources like this! Consider supporting and getting more amazing pharmacology content! Head on over to meded101.com/nurse